Developmental Neuropathology
Chapter 10: Chiari Malformations
Chiari malformations: first described by Hans Chiari in the late 19th century, it encompasses a series of hindbrain deformities associated with hydrocephalus.
Four types:
Chiari I - cerebellar tonsils extend into the upper cervical canal.
Chiari II - displacement of cerebellar vermis into the upper cervical canal with anomalies in the midbrain, pons, and medulla.
Chiari III - displacement of cerebellum into cervical or low occipital encephalocele.
Chiari IV - absence of cerebellum (from secondary destruction, term obsolete)
Chiari I malformations are not really herniation syndromes, although chronic herniation is sometimes called Chiari I. Pathology is distinct from herniation.
Chiari II malformations are also called Arnold-Chiari malformations, although the use of the name Arnold is not really correct.
Epidemiology
- Chiari I malformations - no incidence available, but more detected since MRI availability
- Chiari II - incidence parallels lumbosacral myelomeningoceles, with slight female predominance
- Chiari III - very rare
- Risk factor for Chiari II includes maternal vitamin A deficiency
Embryology and Genetics
- Chiari I is a primary malformation and not a herniation syndrome
- Chiari II embryology is not yet understood
- Chiari III is an encephalocele (previously discussed)
- No clear defined genetic basis for Chiari malformations
Clinical features
Chiari I
- usually presents in teenage to early adult years with neck pain, sometimes torticollis or retrocollis
- arm pain if syringomyelia associated
- brainstem and cerebellar signs depend on structures involved
- in young patients, sleep apnea, near SIDS, stridor, feeding difficulties
- eye movement abnormalities, including oscillopsia and nystagmus
- downbeat nystagmus - suspect problem in cranio-cervial/pontomedullary junction
- torsional nystagmus - syringomyelia/syringobulbia
- dysphagia and aspiration - lower cranial nerve involvement
- imbalance, vertigo, truncal ataxia - vestibulo- and spinocerebellar system involvement
- 40-75% have associated syringomyelia, resulting in spinal cord symptoms
- commonly starts at C4-C6
- symptoms often start affecting crossing sensory fibers (cape-like distribution of loss of pain and temperature sensation in the arms and shoulders)
- anterior horn cell compromise can result in weakness, amyotrophy, areflexia
- with progression, can result in long tract signs
- scoliosis can be the earliest sign in children

Source: http://www.dizziness-and-balance.com/
Chiari II
Chiari III
- poor prognosis, lifespam days to weeks
- symptoms related to hydrocephalus and brainstem abnormalities
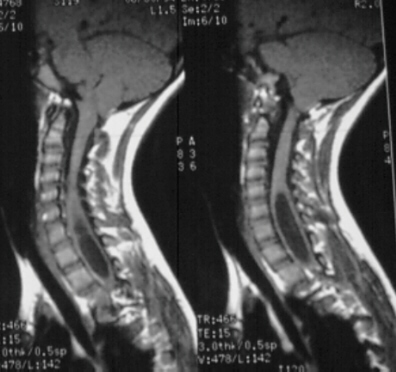
MRI, especially sagittal images, are best for detecting Chiari malformations and syringomyelia
- can be asymptomatic, symptoms more variable and broad than previously believed
- significance of low-lying tonsils questionable - retraction with age
- cut-off in first 10 years - 6mm below the foramen magnum
- cut-off from 10-30 years - 5mm below foramen magnum
- cut-off after age 30 - 4 mm below foramen magnum
- herniations >12mm are almost invariably symptomatic
- syrinx can also be quite large with little symptoms
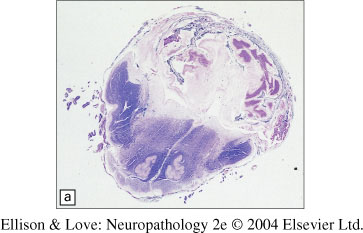
Macroscopy and Histopathology
- cerebellar tonsils below the foramen magnum, usually 1cm or more
- cerebellar tissue at the cervical level can be firm and sclerotic
- acute change of softening and necrosis is rarely present
- remainder of cerebellum is normal
- Chiari I (image at right)
- (in 40%) syringobulbia, hydromyelia, or syringomyelia
- also can have hydrocephalus
- Chiari II
- in 95% with myelomeningoceles
- displacement of vermis (and sometimes inferior lateral cerebellar hemispheres) below foramen magnum
- elongated 4th ventricle, pons, and medulla partially within the spinal canal
- kinked lower medulla
- small posterior fossa with scalloping and erosion of the posteromedial petrous pyramids
- cerebellum can extend lateral and even ventral of brainstem to midline
- beaking (fusion) of the inferior tectum and cranial nerve abnormalities rare
- hydrocephalus is common
- enlarged thalamic massa intermedia
- cerebral periventricular heterotopia, polymicrogyria, pachygyria may be present
- lacunar lucencies in the skull (Luckenschädel) in 85% cases
- cord can also show hydromyelia and/or syringomyelia (hydrosyringomyelia)
- partial (diastematomyelia) and complete (diplomyelia) duplications of the cord can also be seen
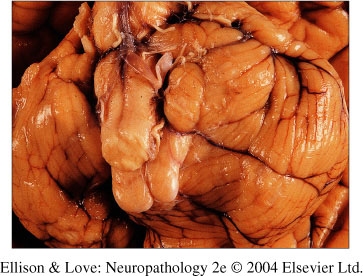
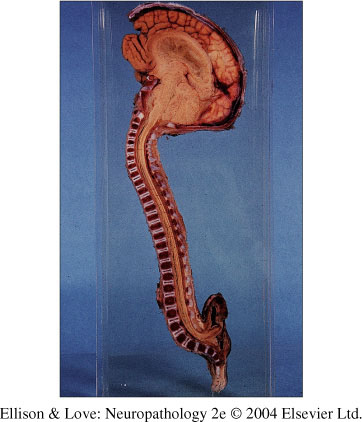
Chiari II malformation.
Note the beaked tectum, hydrocephalus, and lumbosacral myelomeningocele.
Note beaked tectum and elongated brainstem
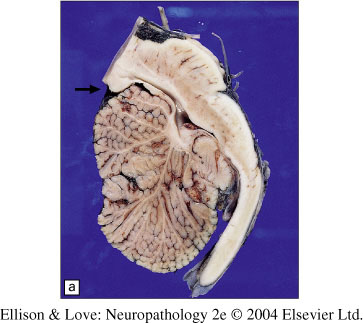
Herniated cerebellar folia showing sclerosis
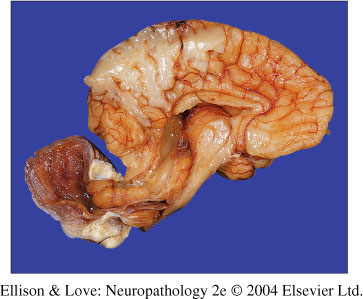
- Chiari III
- defined subtype of encephaloceles
- overlying bony defect (upper cervical vertebrae C1-2 and basal components of the occipital bone of axial and not neural crest origin)
- protrusion of meninges and brain (cerebellum)
- sporadic and rare, unlike syndrome-based occipital encephaloceles which involve squamous bone of neural crest origin and occipital cortical herniation
- small, distorted cerebellum
- brainstem can be distorted
- compromised course of cranial and cerival nerve roots, posterior fosa vasculature, and intrinsic structures of the brainstem and cerebellum
- dysplastic and degenerative changes in the cerebellum, but intact brainstem
- can also have syringobulbia, syringomyelia, and hydrocephalus
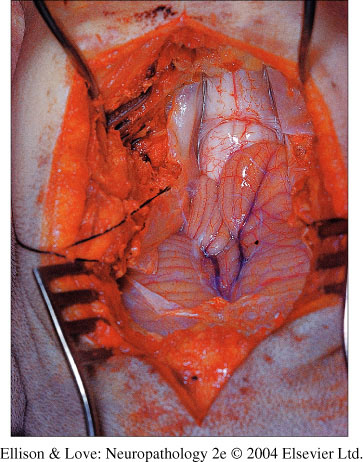
Chiari III malformation
Note cerebellum herniating into the occipitocervical encephalocele
Differential diagnosis
- Chiari I
- clinically, ddx includes MS, SMA, ALS, mononeuropathy multiplex, cervical degenerative disk disease
- imaging resolves these
- difficulty is when there is significant clinical findings but only mild imaging findings
- spinal cord cavities can be hematomyelia, inflammatory (necrotizing myelopathy), metabolic (Leigh disease), neoplastic (astrocytoma, ependymoma)
- NF1 and von Hippel-Lindau can have syrinx
- Chiari II/III
- short differential
- should screen every myelomeningocele for Chiari II
- Chiari III diagnose by MRI
Pathogenesis
Chiari I
- unknown
- developmental anomaly and not herniation
- pathogenesis of associated cord changes also not known
Chiari II - many theories exist as to pathogenesis
- Hydrodynamic theory
- incrased ICP in development pushing down cerbellum
- except the Chiari II occurs BEFORE the hydrocephalus
- Cord tethering
- tethering of the cord causing Chiari II
- course of nerve roots and experimental studies do not support this
- primary defect in neurulation
- primary defect in mesenchyme surrounding posterior fossa
- abnormal growth of posterior fossa forcing cerebellum to develop caudally
- abnormal fluid dynamics at the site of open myelomeningocele and slower resorption displacing the cerebllum downwards
- this theory is gaining support from in utero fetal meningomyelocele repair observations
- observed resolution of Chiari II after closure of the caudal defect
Chiari III
- primary neural tube closure defect
- involves region that rarely shows such a defect