Developmental Neuropathology
Chapter 11: Dandy-Walker Malformation
Dandy-Walker malformation (DVM): well described, but poorly defined. Features exist on a spectrum including
1. cystic dilatation of the 4th ventricle
2. cerebellar vermis abnormalities (hypoplasia to aplasia)
3. enlargement of posterior fossa
4. elevation of the tentorium and transverse sinus
5. hydrocephalus
Can also find lack of patency of one or more foramina of the 4th ventricle.
Dandy-Walker variant (DWV): anteriorly rotated cerebellar vermis with or without dilatation of the 4th ventricle. Unclear if this is separate entity or just mild DWM.
Epidemiology
- precise incidence unknown
- accounts for 3-4% of cases of hydrocephalus
- 1 in 5000 liveborn infants
- diagnosis in infancy and between 10-20 years, or even in adulthood
- 1.5-2 F : 1 M
- associated with isotretinoin use during pregnancy
Embryology
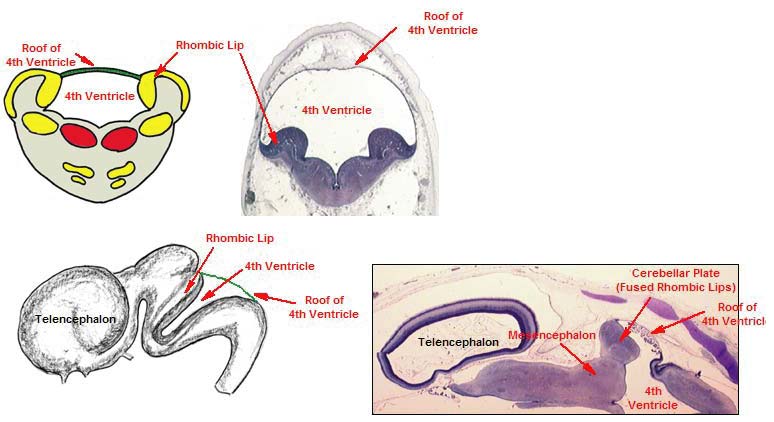
Source: http://isc.temple.edu/neuroanatomy/
- cerebellar development occurs from 3wks GA to postnatally
- cerebellum develops from the fusion of the alar plates of the first rhombomere at 3-4wks GA
- growth of midline components (vermis) occurs at 3rd month GA
- development of the roof of the 4th ventricle (and choroid plexus) is key to development of DWM - area membranacea superior and area membranacea inferior - rostral and caudal regions of the roof of the 4th ventricle
- foramen of Magendie forms at 8 wks, foramen of Luschka later
- area membranacea superior becomes the choroid plexus when the vermis forms
- delayed or blocked foramen of Magendie and/or persistence and thickening of the area membranacea superior implicated in DWM and animal models
- mouse models are key to present understanding:
- isthmic organizer (IsO) denotes boundary midbrain-hindbrain, and establishes anterior limit of cerebellum
- posterior limit not as well understood, may involve Bmps and Shh.
Genetics
- Most cases are sporatic
- infrequent familial cases associated with syndromes
- DWM with mental retardation and spastic paraplegia
- DWM with macrocephaly, facial dysmorphism, brachytelephalangy, and myopia
- Ritscher-Schizel (3C) syndrome - DWM with craniofacial and cardiac abnormalities
- Trisomy 9, 13, and 18 have been reported to have DWM
Clinical features
- most common symptom is hydrocephalus at birth or in infancy
- head size may be large or normal
- cerebellar signs uncommon, signs of increased ICP more common
- mental retardation, but 75-80% have normal intelligence
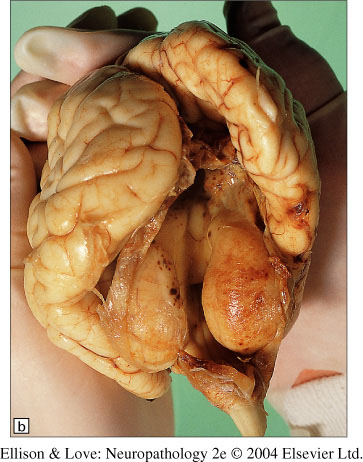
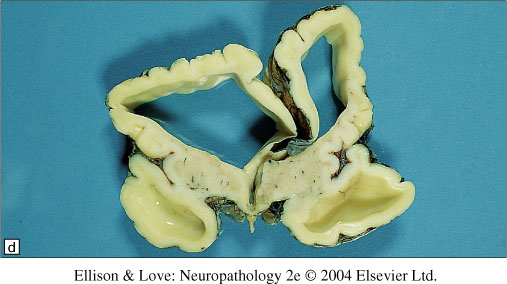
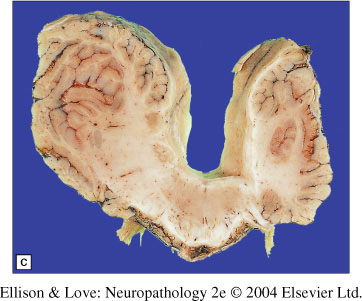
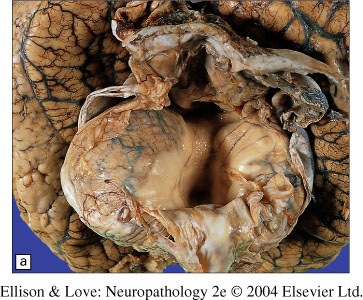
Macroscopy
- cystic dilatation of the 4th ventricle
- cyst composed of posterior medullary velum stretched into a CSF-filled membrane
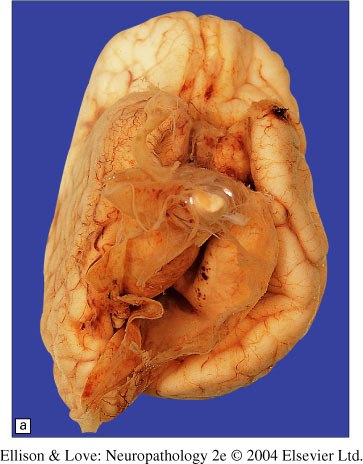
- vermis can be hypoplastic or absent
Note absent vermis, dilated 4th ventricle, and thickened meninges.
- upward displacement of the tentorium and sinuses
- hydrocephalus with dilatation of the aqueduct of Sylvius
- foramina can be open or closed
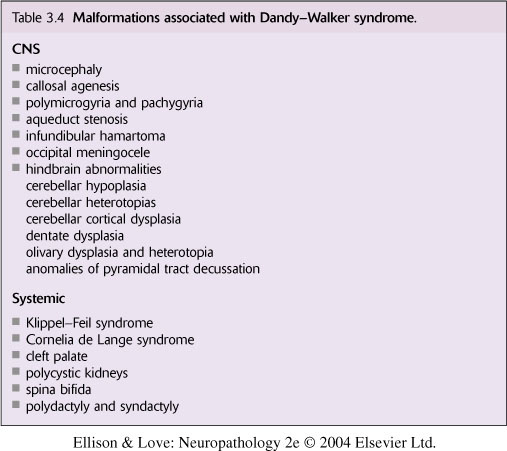
- other associated CNS abnormalities:
- gyral abnormalities, heterotopia, polymicrogyria/agyria/microgyria, malformed inferior olives, cerebellar foliar abnormalities and heterotopias, partial/complete absence of corpus callosum
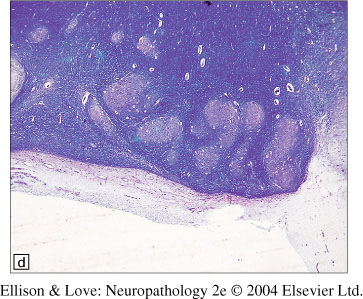
Histopathology
- major findings are seen in gross pathology
- microscopic examination of the posterior fossa cyst shows outer pia arachnoid layer and inner ependymal layer, with microscopic collections of cerebellar tissue
Note fragmented dentate in this case of Dandy-Walker malformation.
Differential diagnosis
- posterior fossa arachnoid cysts - intra-arachnoid
- Arnold-Chiari malformation - shallow posterior fossa, not enlarged
- Joubert syndrome - typically lacks cystic changes, molar tooth sign on MRI, clinical features of respiratory and eye movement abnormalities unlike DWM