Developmental Neuropathology
Chapter 12: Cerebellar heterotopia and dysplasia
Very broad category of malformations from small heterotopias to large (less common) structural malformations
Cerebellar heterotopia of infancy
HSC A04-220

- misplaced/disorganized mature neurons, glial cells, or immature neuroepithelial cells
- common in the cerebellum, more than cerebral heterotopia
- developmental cell rests described in up to 50% normal infants (a lot?) and will to some extent disappear or regress, but may persist
- actual heterotopia more in association with genetic syndromes like trisomy 13, trisomy 18, cerebellar hypoplasia, and other migration disorders
- Four distinct histological types:
1. compact groups of mature neurons
2. immature granular cell collections (focal and perivascular)
3. poorly organized mixed cell rests containing mature neurons and immature neuroepithelial cells ("heterotaxia" of Brun)
4. mixed cell rests with normal relationship of the cerbellar cortex represented ("heterotopia" of Brun)
- granular cell collections can collect around vessels, perhaps an extension of the external granular layer along blood vessels
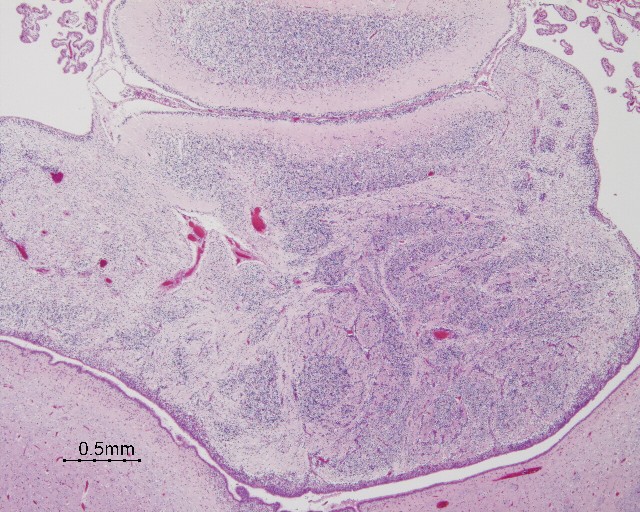
- mixed cell rests occur most frequently
near midline, lateral projections of nodulus of the vermis, roof nuclei, flocculo-nodular lobe
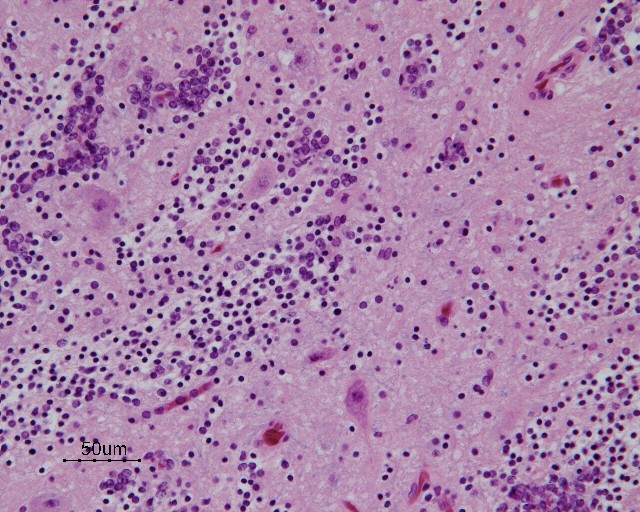
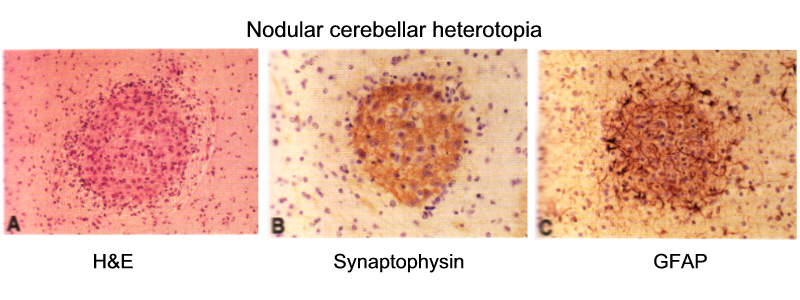
- heterotopic nodules often contain mature neurons surrounded by astrocytes
- dentate nucleus abnormalities can express as:
- simplified C-shaped structure
- multiple detached islands of grey matter
- can occur in isolation or associated with other CNS malformations
- frequency of minor cerebellar heterotopia with regression suggests minimal clinical significance
- persistence may have etiologic relationship with neuroectodermal tumours (cerebellar medulloblastoma)
Cerebellar dysplasia associated with neurodevelopmental syndromes
- more extensive dysplasias involving the hemispheres, vermis, or entire structure
- associated with more generalized malformations of the cerebrum
- symptoms of seizures and cognitive defects often related to cerebral malformations
- unclear what symptoms actually relate to the cerebellar defects
- examples of such disorders include:
- Type II Lissencephaly - Walker-Warburg syndrome, Muscle-eye-brain disease, Fukuyama congenital muscular dystrophy
- Type I Lissencephaly
- Meckel-Gruber syndrome
- Tectocerebellar dysraphia
- Zellweger syndrome - peroxisomal disorder with migrational abnormalities
- Dandy-Walker malformation
- Joubert syndrome
- rhomboencephalosynapsis
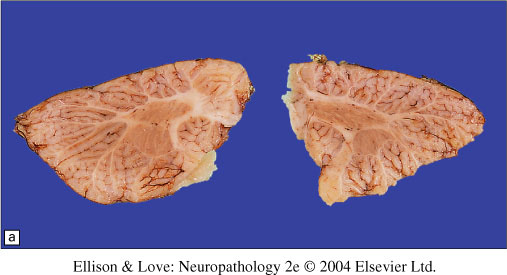
Rhomboencephalosynapsis
- rare malformation with vermian aplasia or hypoplasia with fusion of the cerbellar hemispheres
- no 4th ventricle midline defect
- associated with fusion of the thalami and/or inferior colliculi
- associated with septo-optic dysplasia
- frequency of 0.13%, diagnosed by MRI in children and adults
- clinically associated with facial and non-cranial abnormalities, hypoplasia of the temporal lobes, fornix, and anterior commissure, incomplete agenesis of the corpus callosum
- usually die in childhood, but may survive to 3rd decade
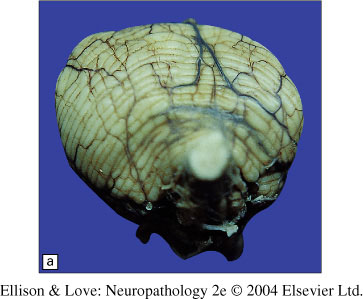
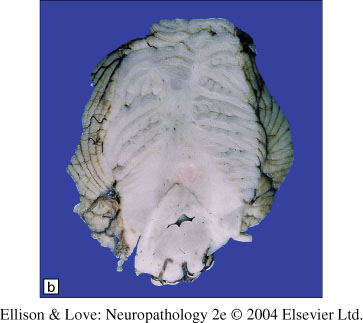
- Gross and histology:
- small, pear-shaped cerebellum
- aplasia of the vermis
- apparent fusion of the cerebellar hemispheres
- constricted diamond-shaped 4th ventricle, not obstructed
- closely apposed dentate nuclei, better formed caudally than rostrally

- hydrocephalus may exist due to aqueductal atresia
- can have absence of olivary nuclei
- Pathogenesis:
- dorsal patterning defect in the "isthmic organizer" (IsO), studied in mouse models