Developmental Neuropathology
Chapter 13: Brainstem malformations
Olivary heterotopia
- displacement of the inferior olivary nucleus dorsal-laterally due to faulty migration
- rare microscopic anomaly often associated with other malformations and genetic mutations
- Miller-Dieker syndrome (pachygyria) from LIS-1 mutation
- X-linked neonatal PDHC deficiency and cerebral lactic acidosis
- Dandy-Walker malformation
- megalencephaly
- trisomy 13
- no associated imaging or laboratory abnormalities
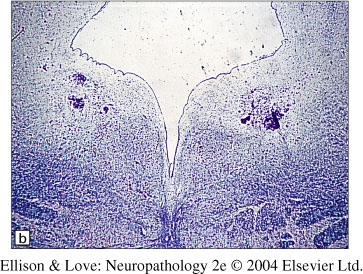
- Pathological findings
- olivary heterotopias usually laterally in the rostral medulla, sometimes medial
- mature olivary neurons and neuropil can form nodules or serpiginous structures reminiscent of the olives
- can be single or form multiple islands
- actual inferior olive can be dysplastic, poorly folded, thickened, or fragmented and smaller than normal
- Embryology and pathogenesis
- neural precursors start from the rhombic lip before the 3rd month GA
- arrest of migration during the 1st trimester
- same time period as pachygyria
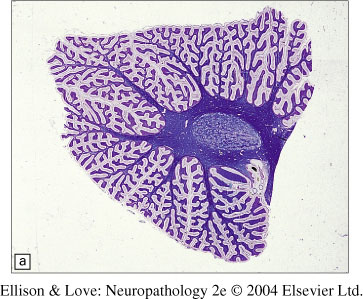
Dysplasias of the dentate and olivary nuclei (DOD)
- ontogenetically related nuclei
- often overlooked, very rare
- associated with bigger anomalies
- agenesis of corpus callosum
- Zellweger syndrome
- cerebellar hypoplasia
- one group has developmental delay, seizures (tonic), burst-suppression on EEG in infancy, autosomal recessive inheritance
- Embryology and pathogenesis
- both the dentate and olivary nuclei are derived from the rhombic lip
- maturation of the structures by 7th month GA
- failure of normal development due to interference with late neuroblast migration or differentiation of precursor cells
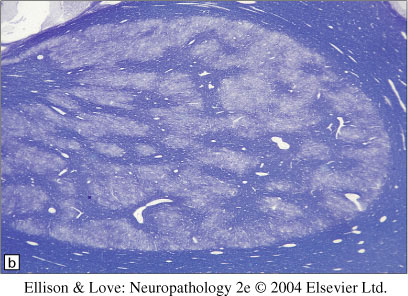
- Pathological findings
- macroscopically, can only be detected by careful observation in mature brains (hard to see in immature brains
- histological findings differ with the dysplasia:
- thanatophoric dysplasia - excessive folding of dentate and olivary nuclei
- cerebellar aplasia/hypoplasia - poorly convoluted olives, simplified/fragmented dentate
- Joubert syndrome - C-shaped olives
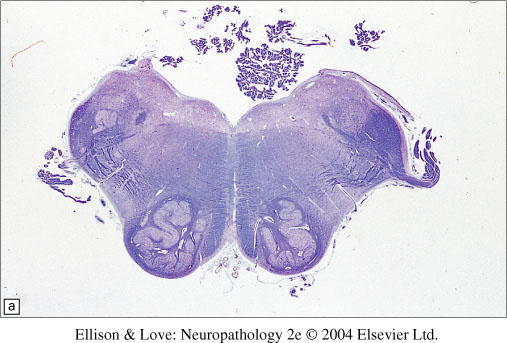
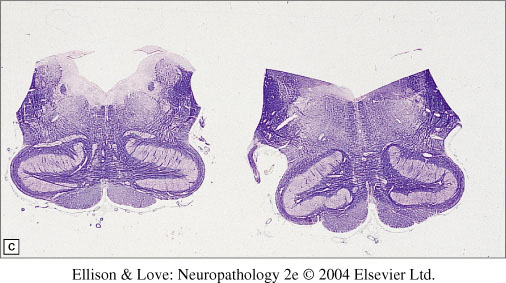
- trisomy 13/Zellweger syndrome - dorsally-thickened, C-shaped olives with loss of folding, peripheral margination of neurons and discontinuities in the ribbon
Olivary dysplasia in Zellweger syndrome
Dentato-olivary dysplasia with intractable seizures in infancy
- dentate and olivary malformation with intractable neonatal seizures, EEG with burst-suppression, and poor prognosis
- also called "early epileptic encephalopathy with suppression burts and olivary-dentate dysplasia"
- affects both sexes, presenting in neonatal period
- most cases sporadic, one case suggests autosomal recessive inheritance
- clinical symptoms
- hypotonia, poor feeding, frequent seizures in first day of life
- normal clinical examination
- seizures intractable to medical management
- predominant seizure type is tonic seizures
- gross developmental delay, normocephalic
- profound handicap, survival <3yrs, usually dying of respiratory causes
- MR/CT normal
- EEG burst suppression, EPs normal, metabolic studies normal
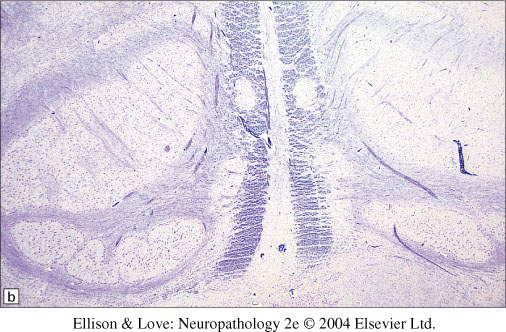
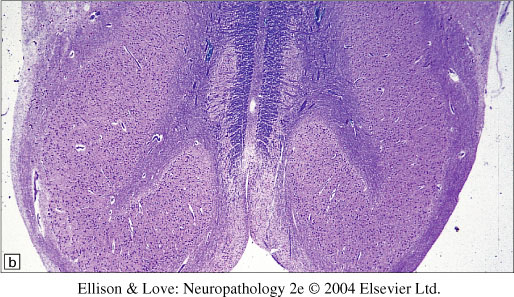
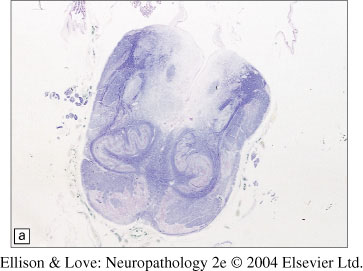
- Histological findings
- small brain, loss of outline of the olive and dentate, with solid globose appearance of the dentate nucleus
- on histopathology can show cortical atrophy and ischemic lesions
- solid dentate with indistinct hilum
- coarse hook-shaped inferior olives without undulation
- Differential diagnosis
- difficult, since unable to detect on imaging
- diagnosis depends on EEG pattern and seizure types (lack of myoclonus, pattern of tonic seizures early in course
Möbius syndrome
- described in 1888 by Möbius
- facial diplegia with bilateral abducens palsy
- sometimes involves more cranial nerves, especially lower cranial nerves to the tongue (CN9-12)
- may be associated with in utero exposure to cocaine
- mostly sporadic occurrence, some familial with autosomal dominant, recessive, and X-linked inheritance reported
- linkage to chromosomes 13q12.2-12, 3q21, and 10q21 found
- Clinical features
- mask-like face, bilateral internal strabismus
- drooling, speech difficulty
- normal intelligence usually
- sometimes unilateral
- some have skeletal abnormalities - talipes, syndactyly, arthrogryposis, small limbs, Poland anomaly (absent pectoralis major and symbrachydactyly)
- feeding problems in infancy, sometimes with micrognathia
- if severe, respiratory and bulbar problems can be fatal in neonatal period
- need to address issues of maternal bonding, but facial mobility improves with age
- Pathological findings
- No macroscopic findings
- On histology, heterogeneous findings, 4 types:
1. myopathy
2. primary peripheral nerve involvement
3. aplasia/hypoplasia of cranial nerve nuclei, plus other brainstem anomalies, e.g., olivary dysplasia
4. focal necrosis and calcification of brainstem nuclei
- Pathogenesis
- believed that the midline and paramedian zones of the developing brainstem are poorly vascularized and more vulnerable to injury
- proposed vascular/ischemic injuries in utero or perinatally, e.g., cocaine, alcohol
- similar findings have been observed in some homeobox gene defects