Developmental Neuropathology
Chapter 14: Spinal cord lesions
Many variable disorders with poor understanding of pathogenesis. They often occur in combination with, e.g., meningomyelocele or Chiari I malformation.
Hydromyelia: dilation of central canal from incomplete fusion of the posterior columns or persistence of the primitive large canal of the embryo. Can be focal, esp. lumbar. Often isolated incidental finding in neonatal autopsy. Often found in association with Chiari I or II malformations.
Syringomyelia: dilated, glial-lined cavity in spinal cord. Syringobulbia in the brainstem. This cavity does not communicate with the central canal, and usually is between the dorsal columns unilaterally or bilaterally along the side of the cord.
Malformations associated with syringomyelia and hydromyelia
- Cranio-cervical junction
- Chiari malformation
- basilar impression
- "tight" cisterna magna
- rhomboencephalic malformation
- Spine and spinal cord
- fusion of vertebrae
- Klippel-Fiel anomaly
- spina bifida complex
- tethered cord syndrome
- diastomatomyelia
- myelomeningocele
Diplomyelia: duplication of the spinal cord
Diastomatomyelia: coexistence of two hemicords, at variable levels, causing splaying of the posterior vertebral elements. Results in neurological deficits in lower limb or perineum.
Hemicords can be separated by rigid osseocartillaginous septum (Split cord malformation type I) or in a single dural sac separated by a fibrous median septum (Split cord malformation type II).
Both diplomyelia and diastomatomyelia can occur concurrently. Usually symptomatic in adults and not in children. Can be incidental finding on neuroimaging.
Triplomyelia: triplication of the spinal cord extremely rare
Spinal tract defects: include aplasia of the corticospinal tracts or dorsal columns, asymmetric crossing of spinal tracts, or fusion of tracts across the midline.
Risk factors
- syringomyelia can occur post-traumatically
- hydromyelia and syringomyelia can accompany tumours of the spinal cord
- fused cord with loss of tracts seen in caudal regression syndrome associated with maternal diabetes
Genetics
- syringomyelia seen in Hajdu-Cheney syndrome and Crouzon syndrome
- familial syringomyelia has been reported as autosomal dominant, with basilar impression, scoliosis, enlarged sagittal diameter of the cervical canal, pyramidal tract findings in lower limbs, ectopic cerebellar tonsils
- diastematomyelia is rare and usually nonsyndromic and sporadic, but some familial cases (variable expressivity, mostly reported in females ?X-linked dominant with lethality in males)
Clinical features
- hydromyelia
- hydromyelia often associated witih communicating hydrocephalus
- can be asymptomatic or associated with mild spastic paraparesis, legs more than arms, depending on level of hydromyelia
- compression of the lateral columns contributes to symptoms
- syringomyelia
- depends on location and severity of syrinx
- can start with segmental signs of muscle wasting
- develops to segmental muscle weakness and bilateral pain and temperature loss (from crossing fibers)
- split cord abnormalities
- symptoms usually associated with long tract signs
- arthrogryposis and fetal akinesia syndrome
- arthrogryposis reflects severe fetal limb immobility
- can be effect of CNS or PNS genetic conditions
- can also be due to lower motor neuron, motor end-plate, or muscle disorders
- severe cases are associated with growth retardation, craniofacial abnormalities, limb abnormalities, pulmonary hypoplasia, short umbilical cord, polyhydramnios
- e.g. type I Pena-Shokeir syndrome - autosomal recessive
Imaging and biochemistry
- MRI is the modality of choice for diagnosis
- syringomyelic cysts have higher protein content than hydromyelic cavities
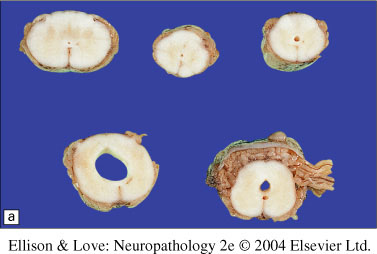
Macroscopy
- Hydromyelia is usually a symmetric dilatation of the central canal that can extend as rostral as the 4th ventricle and as caudal as the conus medullaris
- Syringomyelia is asymmetric, but usually between the dorsal columns, and usually in the cervical cord
- Diastematomyelia can show a bony, cartilaginous, or ligamentous protruberance partially dividing the cord, usually from the dorsal aspect, and in the distal spinal cord extending over <10 segments
- Diplomyelia is very rare, but shows a mesenchymal separation between the duplicated cords
Histopathology
- Hydromyelia
- can be lined with ependymal cells, sometimes flattened, sometimes denuded leaving a glial parenchymal lumenal lining
- often only in focal areas
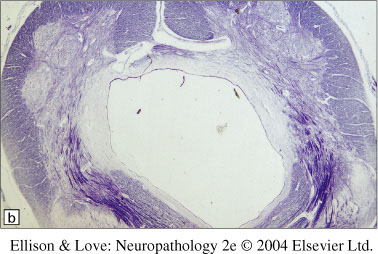
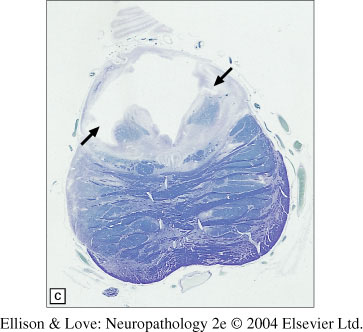
- Syringomyelia
- commonly through thoracic cord, rarely in lumbar cord
- single cavity can be merged with central canal, or two cavities
- irregular tract pathways, can cross structures
- reactive glial lining, with adjacent gliotic tissue with Rosenthal fibers and loss of neurons or myelinated fiber tracts depending on affected tissue
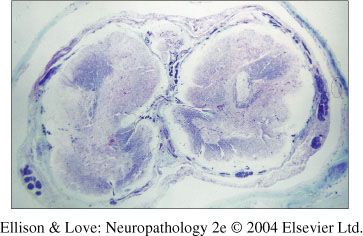
- Diastematomyelia
- spectrum of findings:
from duplication of central canal
to duplication of dorsal columns
to ventral midline fusion and duplication of all elements
- usually duplicated structures are smaller than normal structures
- defects in various tracts and heterotopias
- defects in descending tracts most common, often seen as asymmetric crossing of the tracts. Unclear clinical significance.
- heterotypic tissues - cartilage or epithelial cysts - can be in isolation of associated with other defects, most commonly in caudal spinal cord and conus medullaris. Unclear clinical significance.
Differential diagnosis
- clinical information important to help in determining cause of syringomyelia - developmental, malformation spectrum, or traumatic/vascular lesion
- common in Chiari I malformations with myelomeningoceles
- trauma can show recent or old hemorrhage with iron deposition, as well as more pronounced gliotic reaction and Rosenthal fiber formation
- glial tumours (astrocytoma, oligodendroglioma, ependymoma) and neuroglial tumours (gangliocytoma) can have syringomyelia or hydromyelia - check MRI and histopathology
Pathogenesis
- hydromyelia/syringomyelia
- pathogenesis debated, and important for possibility of halting process surgically
- malformation if communicating with 4th ventricle and extending along cord, with congenital hydrocephalus
- destructive lesion from developmental disorder if primary syringomyelia, likely due to abnormal CSF hydrodynamics forcing CSF into the cord parenchyma, possibly via enlarged Virchow-Robin spaces
- another hypothesis is that a tight cisterna magna in Chiari malformations may divert CSF into the spinal canal, leading to pressure and syrinx formation