Developmental Neuropathology
Chapter 18: Antenatal disruptive lesions
Classical patterns of neonatal brain injury are:
- combined grey and white matter lesions - intrauterine damage
- isolated white matter lesions - prematurity
- isolated grey matter lesions - perinatal injury
This classical view is not entirely accurate, much more complex than this. "Hypoxic-ischemic encephalopathy" encompasses a large number of pathological findings, including hydranencephaly, porencephaly, schizencephaly, basket brain, cystic or mylticystic encephalopathy, twin-twin transfusions syndrome, arterial infarction, leukomalacia, etc.
HIE Neuropathology
- necrosis/hemorrhage of the white/grey matter
- rapid growth and interference with development of the CNS
- Primary lesions
- wide spectrum of abnormalities ranging from minimal focal infartcts to cavitary lesions
- must consider
(1) ability of immature brain to respond to injury and
(2) fast growing evolution of lesions
- lesional age
- astrocytic and macrophage reactions not prominent or specific prior to 20 wks GA
- insults from 16-22 wks GA - interferes with cortical plate organization, e.g., polymicrogyria, neuronal heterotopia
- later insults - laminar or total necrosis of the cortical plate
- polymicrogyria with necrosis of cortical plate -> persistent insult
- lesional distribution
- sharp demarcation of arterial infarction
- diffuse nature of global perfusion failure
- white vs. grey
- severe necrosis of cerebral mantle results in rim of vascular neuroglial tissue with mineralization, reactive astrocytes, and foamy/hemmosiderin-filled macrophages, thickened leptomeninges with vascular proliferations and neuroglial ectopia
- white matter necrosis leads to hemorrhage and/or calcification, cavitation, and hydrocephalus
- Overproduction of TNF-alpha (tumour necrosis factor alpha) and beta-APP (beta-amyloid precursor protein) are good lesional markers
- Secondary changes
- effects differ with time of insult:
- brain atrophy
- abnormal gyral pattern (pachygyria, microgyria, ulegyria)
- ventriculomegaly
- septal rupture
- atrophy of fibers and tracts
- corpus callosum atrophy
- corticospinal tract atrophy - peduncle and medullary pyramid atrophy
- secondary thalamic atrophy
- secondary striatum and pallidum neuronal alteration and mineralization
- lateral tract atrophy of spinal cord
Spectrum of antenatal HIE
- detected on fetal U/S and MRI
- usually not detectable before 20 wks GA
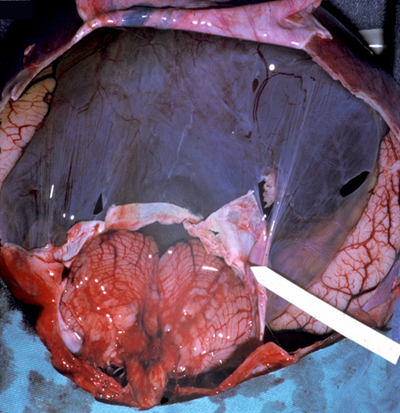
- Hydranencephaly
- "hydro-anencephaly"
- severe, diffuse necrosis of the cerebral mantle leading to ex vacuo hydrocephaly
- cerebral mantle replaced by floating membrane of thickened leptomeninges and the remnant of the underlying necrotic cerebral mantle
- only remaining components: medial temporal lobes, caudal thalamus (posterior circulation), cerebellum (may be cystic also)
- cystic or atrophic olfactory and optic nerves, pituitary tract, basal ganglia
- secondary atrophy of brainstem and spinal cord
- due to internal carotid distribution perfusion failure before 15-16 wks GA
- etiologies include maternal trauma, twin-twin transfusion syndrome, massive hemorrhage, familial vascular malformations (proliferative glomeruloid vasculopathy)
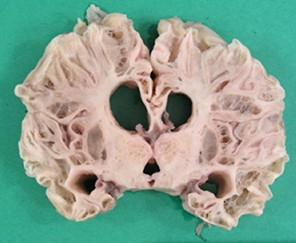
- Porencephaly
- cavitary necrosis of the cerebral mantle of one or both hemispheres (often left)
- usually MCA territory, resulting in septum pellucidum destruction and dilated ventricles

- residual mantle has radial gyri around edges of defect
- residual cortex can be gliotic with dystrophic calcifications and polymicrogyria
- usually contralateral hemisphere partially affected
- in bilateral lesions, only mid-sagittal territories not affected - "basket brain"
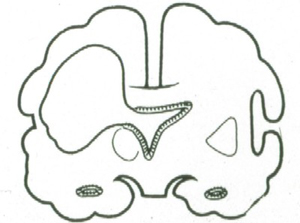
- Schizencephaly
- "cleft" in cerebral mantle without communication with ventricle
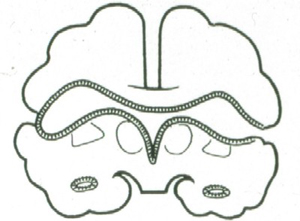
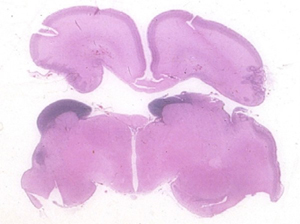
- overgrowth and disorganization of surrounding hemisphere
- edges may seem to fuse (closed lips) or stay apart (open lips)
- Multicystic encephalopathy
- diffuse cortical and subcortical white matter necrosis
- results in lace-like cavities
- late occurring lesion during partuition or first postnatal month of term pregnancy
- can be due to infectious encephalopathy, e.g., CMV, toxoplasmosis, listeria
- can be due to twin-twin transfusion
- Cerebellar cysts
- one or both cerebellar hemispheres
- liquid-filled cavities communicating with 4th ventricle
- associated disruption of the cytoarchitecture and deep nuclei
- Brainstem damage
- various cranial nerve nuclei lesions
- seen in Möebius syndrome, Pierre-Robin sequence, Hanart (aglossia, adactylia), and fetal akinesia deformation sequence (FADS, Pena-Shokeir)
HIE causes and genetic counselling
- hypoxic-ischemic injury as a result of a number of etiologies including materal, placental, or fetal.
- maternal causes:
- direct trauma
- drug abuse
- gas intoxication (CO, butane)
- hypovolemia
- coagulopathies
- placental causes:
- placental insufficiency
- twins
- fetal causes:
- hydrops
- infections
- hemorrhages
- vasculo-occlusive processes
- detailed familial analysis may uncover other siblings with disruptive lesions of other organs
- familial cases of HIE suggest risk factors including vasculopathy, coagulopathy, teratogens, enzyme deficiencies, mitochondrial angiopathies and cytopathies
- unclear etiologies make it hard to reduce HIE