Developmental Neuropathology
Chapter 19: Hemorrhagic lesions
Defined by anatomical location, and circumstance:
- arterial, capillary, or venous
- intravascular hypertension, thrombosis, breakdown of vessel integrity following infarction or trauma
- location of infarct partly dictated by developmental stage
- subdural, subarachnoid
- intracortical, white matter
- choroid plexus
- brainstem/cerebellar
- periventricular - from germinal matrix or white matter
- intraventricular - from ganglionic eminence or choroid plexus
Subventricular zone = subependymal zone = subependymal matrix = germinal matrix
Ganglionic eminence: large aggregate of cells of the subventricular zone along the wall of the lateral ventricle, especially over the immature caudate nucleus
Epidemiology
- In utero bleeding rare
- autopsy studies are biased to worst outcome
- small sub dural, subarachoid and intracerebral hemorrhages are common (20-30% livebirths)
- large intraventricular and posterior fossa hemorrhages - 10-15% livebirths
- choroid plexus hemorrhage usually at >35wks GA and not as severe
- decreasing incidence over time
- incidence of intraventricular/periventricular hemorrhage is inversely proportional to gestational age at birth
- 40-50% infants born at < 26wks GA
- 20% at 26-32 wks
- < 5% at > 32wks
- severity also worse in those of lower GA
- incidence of asymptomatic small subdural/subarachnoid (50%) and choroid plexus (30%) hemorrhages detected on MRI following uncomplicated term births are much higher than symptomatic intracranial hemorrhage (2.7%)
- 60% hemorrhages occur within first 24 hours of life, most within 3-4 days
- highest risk periods are first 3 hours of life, day 2, and day 10 of life
- Risk factors:
- mainly prematurity, with associated RDS
- IUGR
- maternal/fetal sepsis, PPROM, chorioamnionitis
- inconsistent relationship with maternal HTN and preeclampsia
- traumatic delivery is risk factor for subdural hemorrhage
Embryology
- ventricular zone lines fetal ventricle
- ganglionic eminence is C-shaped collection of proliferating cells in the subventricular zone, below the caudate nucleus, along the ventricles down the temporal horns towards the amygdala
- neuronal precursor cells (especially GABAergic interneurons) are produced up to 18 wks GA, then glial precursors
- volume of subventricular zone peaks at 23-25 wks GA
- largely involutes by 38-40 wks GA leaving some cells in the subependymal region
- ciliated ependymal cells appear as the ventricular zone involutes
- large veins in the ganglionic eminence are the source of hemorrhage
Clinical features
- usually clinically occult
- if severe, can be irritable, have decreased LOC, tense fontanel (incr ICP), low HCT (bleed), seizures
- mortality for birth weight < 1500g (30 wks GA) is 30%
- morbidity is 25% of abnormal neurological outcome
- morbidities include:
- hydrocephalus
- cerebral palsy (hemiplegic)
- cognitive delay
- effects difficult to differentiate with PVL
- subdural hematomas have grave consequences if incr ICP or in the posterior fossa
Imaging
- primary diagnostic tool - screening recommended
- grading system based on CT, but not recommended due to radiation effects
- Papile grading system
Grade I: isolated subependymal hemorrhage (SEH)
Grade II: SEH with IVH, no ventricular enlargement
Grade III: IVH with enlarged ventricles
Grade IV: IVH and SEH with extension into brain beyond the ganglionic eminence
- this grading system is now used with U/S
- other grading systems exist
- Three grade system differentiating extent of parenchymal damage:
Grade 1: focal SEH
Grade 2: extension into basal ganglia
Grade 3: extension laterally or superiorly into cerebrum
- germinal matrix vs. white matter hemorrhage
B1 - isolated GMH or choroid plexus hemorrhage
B2 - GMH with IVH, without ventricular enlargement
B3 - GMH with IVH and ventricular enlargement
W1-W4 - white matter hemorrhage from PVL
- MRI findings are more sensitive for small foci of hemorrhage
Laboratory tests
- imaging most important
- screening for etiology, e.g., clotting parameters, antiplatelet antibodies (neonatal alloimmune thrombocytopenia)
- CSF may be bloody, and cytokine levels in the umbilical cord may have some predictive value
Macroscopy
- most useful in acute cases
- subdural and subarachnoid hemorrhages usually thin


- germinal matrix hemorrhage located in the anterior ganglionic eminence over the caudate, often unilateral and asymmetric, associated with IVH
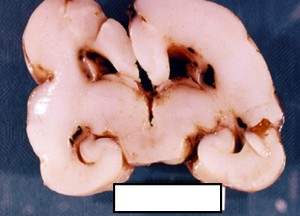

- hemorrhagic conversion of ischemic lesions more bilateral and symmetric in posterior white matter
- IVH seldom due to extension of white matter hemorrhage
- large intraventricular blood degrades slowly
- progresive hydrocephalus in 20%
- lateral extension of germinal matrix hemorrhage can damage maturing brain parenchyma
- resolution of the hematoma (few months) results in focal, smooth-walled cyst adjacent to lateral ventricle
Histopathology
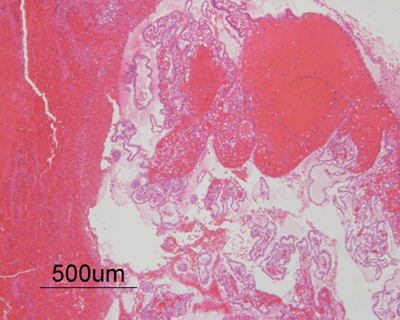
- blood cells intermingle with with parenchyma, especially noncohesive germinal matrix cells
- identification of disrupted blood vessel helps understand process, but not diagnosis
- hemorrhaging conversion of ischemic lesion - petechial hemorrhages, not usually hematoma
- hemosiderin apparent as early as day 3 after bleed
- reactive astroglial and microglial changes are subtle, inflammation mild
- surrounding necrotic tissue if hematoma large enough to cause secondary infarction
- after 1 month, only outer 1-2mm of a hematoma will have organized
- after months, residual hemosiderin and mineralization may be seen in the ventricle wall
- hydrocephalus in aborted fetuses
- careful investigation for blood blocking cerebral aqueduct important for counselling
Experimental models
- studies of immature rabbits, dogs, cats, and sheep help us understand the mechanism of germinal matrix hemorrhage
- showed that fluctuations in arterial and venous blood pressure, and not asphyxia alone, can cause periventricular hemorrhage
Pathogenesis
- differs between types of bleeds
- in premature babies, germinal matrix hemorrhage occurs at thin-walled veins running through the germinal matrix, which does not offer good structural support to the vessels
- rupture can be due to mechanical distortions, but more frequently from fluctuations in intravascular and intracranial pressures
- endogenous fibrinolytic activity in the germinal matrix may contribute to the vascular fragility
- blockage of the aqueducts usually resolve, but if scarring occurs, there can be progressive ventricular enlargment
- bleeding can also be due to arterial reperfusion following ischemia
- also due to distal occlusion by thrombus or hematoma
- focal subarachnoid hemorrhage from rupture of small vessels of rare clinical significance
- clinically significant subdural hematomas tear into the falx cerebri, tentorium, or sinuses