Developmental Neuropathology
Chapter 25: Kernicterus
Kernicterus: (bilirubin encephalopathy) characterized by jaundice, acute neurological dysfunction with specific neuronal damage resulting in athetosis, spasticity, hearing deficits, and mental deficits.
Yellow staining of brain structures first described by Hervieux in 1847, later associated with neonatal jaundice by Schmorl in 1903.
Epidemiology
- although neonatal jaundice is common, progression to kernicterus is rare
- incidence in US of 5 cases per year
- boys more susceptible than girls
- inverse relationship to gestational age at birth
- Risk factors:
- hyperbilirubinemia in the neonatal period (defective bilirubin metabolism)
- predisposing conditions include:
- extreme prematurity
- hemolytic disease secondary to isoimmunity to Rh, ABO, or other blood group factors
- hereditary diseases, e.g., glucose-6-phosphate dehydrogenase deficiency (G6PD), Crigler-Najjar syndrome (especially type I), Arias syndrome, Gilbert disease, Lucey-Driscoll syndrome (transient familial neonatal hyperbilirubinemia)
- breastfeeding
- sepsis
- intestinal disorders (pyloric stenosis, intestinal obstruction, Hirschprung disease)
- congenital hypothyroidism
- infant of diabetic mother
- East Asian/Mediterranean descent
- excessive bleeding in the newbord period
Clinical features
- clinical features are well defined, but not all neonates will exhibit these features
- Acute phase:
- stupor, hypotonia, poor suck
- few days later - opisthotonus and retrocollis
- few days later - hypotonia
- can be accompanied by fever without evidence for infection
- Silent stage:
- hypertonia, hyperreflexia
- persistent righting reflex
- psychomotor retardation
- Chronic stage:
- movement disorder, typically athetosis - slow writhing movements, arm more than legs or face
- swalowing and phonation difficulties
- other movement disorders: chorea, dystonia, ballismus
- vertical gaze palsy, hearing disturbances (especially high frequency range)
- mental retardation
- Imaging:
- high signal intensity of the globus pallidus on T2 weighted MRI
- Laboratory findings:
- high serum bilirubin
- other tests for etiology, e.g., ABO, G6PD, sepsis
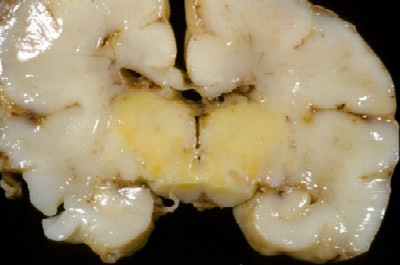
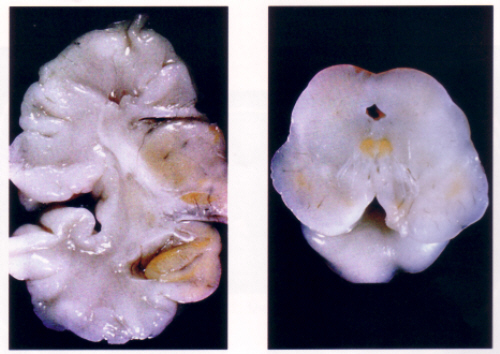
Macroscopy
- on the surface, the cerebellar flocculus may appear yellow
- on section, yellow discolouration of the globus pallidus, mammilary bodies, subthalamic nucleus, and thalamus
- no involvement of the cerebral or cerebellar cortex except for a few areas including the hippocampus, subiculum, induseum griseum, uncus, and flocculus
- in the brainstem, involved nuclear groups include the substantia nigra, CN III nucleus, CN IV nucleus, vestibular nucleus, other nuclei along the 4th ventricle, inferior olivary nuclei, dentate and other cerebellar roof nuclei
- most consistent finding is atrophy of the globus pallidus, but also the hippocampus, subthalamic nucleus, brainstem, thalamus, and hypothalamus
Hisopathology
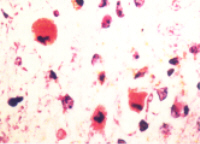
- primary target of bilirubin encephalopathy is the neuron
- intracellular bilirubin only identified in very high bilirubin concentrations, and even then is difficult
- changes are acute necrosis, similar in appearance to hypoxic-ischemic injury or hypoglycemia
- dead neurons may become encrusted in calcium or iron salts
- protoplasmic and/or fibrillary astrocytes appear in a few days
- structures susceptible to neuronal damage:
- medial and lateral nuclei of the pallidum, "red zone" of the substantia nigra, subthalamic nucleus, mammilary bodies, induseum griseum, H2 and H3 of the hippocampal formation (more than H1 and H5), CN III nucleus, interstitial nucleus of Cajal, CN IV nucleus, CN VIII, central pontine and pontine reticular formation, inferior olivary, dentate, and cerebellar roof nuclei
- neuronal necrosis of spinal cord has been reported, but no reports of yellow staining of the cord
- chronic lesions
- neuronal loss and gliosis
Biochemistry
- basic problem of inability of liver to conjugate the bilirubin
- requires hepatic enzymes including uridine-diphosphate (UDP) glucuronosyl transferase
- variables include gestational age, albumin concentration, bilirubin load, pH, sepsis, hypoxia-ischemia, integrity of blood brain barrier
Differential Diagnosis
- other CNS disorders can cause similar symptoms in a sick neonate, including HIE, sepsis, metabolic diseases, increased ICP from tumour, malformations, or infections
- gaze disorders and extrapyramidal movements present after one year age, but can also be due to tumour, infection, genetic, metabolic, degenerative, or toxic diseases