Study Group Notes - Chapter 57 – Spinal Cord Vascular
Disease
Vascular anatomy
of spinal cord:
 Embryonic arterial supply derived from
radicular arteries entering at each spinal level, dividing to follow dorsal
and ventral roots
Embryonic arterial supply derived from
radicular arteries entering at each spinal level, dividing to follow dorsal
and ventral roots- Ventral roots join to form anterior spinal
artery
- Irregular anastomoses in posterior form paired
posterior spinal arteries
- Circumflex arteries (arteria vasocorona) connect
anterior and posterior systems
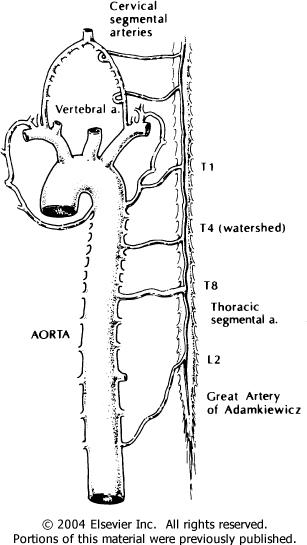
- Development, 5-8 radicular arteries become
predominant
- Great artery of Adamkiewicz follows a lower thoracic or upper lumbar nerve root,
and supplies the lower thoracic cord and lumbar enlargement
- Lower segmental arteries supply the sacral cord, conus
medullaris, and cauda equine
- Plexus from branches of ascending cervical and
vertebral arteries supplies cervical and upper thoracic cord
- Traditionally, midthoracic cord considered most
vulnerable, but new studies find lumbosacral cord moreso
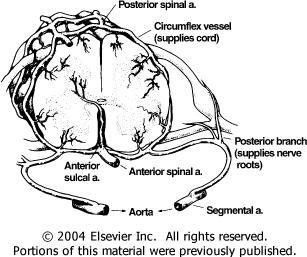
Anterior spinal
artery à anterior sulcal artery à supplies spinal grey matter, anterior and
lateral funiculli, each to only one hemicord, spacing proportional to numbers of
neurons at cord level
i.e. thoracic
segments have greatest distance between arteries
Posterior spinal
arteries à penetrating branches à supplies dorsal columns and extreme dorsal
horns (1/3 of cord in cross-section)
Circumflex
anastomotic vessels à superficial white
matter
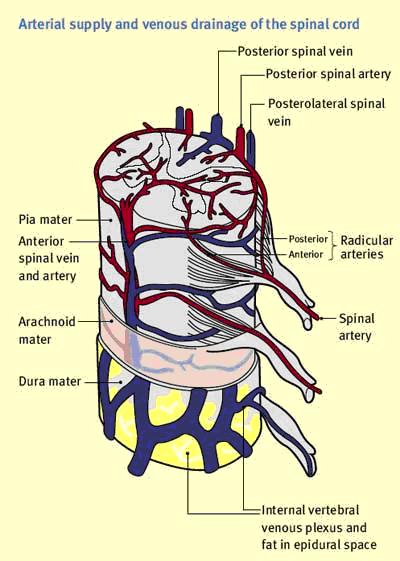
- Venous system parallels arterial
supply.
- Radial veins à coronal plexus
- Deep parenchymal veins à central sulcal vein in median fissure
(from both hemicords)
- Sulcal veins have intersegmental
anastomoses
- Posterior median spinal vein is prominent within the
extramedullary venous channels
- Vena radicularis magna – drains everything at the level of the lumbar
enlargement
- Posterior radicular veins most prominent in cervical
levels
- Venous blood from cord enteres epidural and
paravertebral venous pexuses to form a valveless system from sacrum to occiput
(Batson’s plexus)
Spinal cord
ischemia:
- <1% of all acute strokes
Clinical
presentation and course
- Weakness, numbness, pain, urinary
complaints
- Can progress over hours, or suddenly
- Vulnerable thoracic cord à paraparesis more common than
quadriparesis
- Numbness and paresthesias parallels (sometimes
precedes) weakness
- Radicular back pain common
- Visceral referred pain
- Urinary retention (or bladder/bower incontinence after
initial spinal shock)
- Examination: flaccid paresis, decreased reflexes…
develops into spasticity, hyperreflexia, upgoing plantars if lesion above
lumbar spine
- Posterior spinal artery syndrome rare – preserved
strength and reflexes
- Sensation:
- ASA – impaired pain and
temperature
- PSA – impaired touch, vibration,
proprioception
- Small lesion – partial Brown-Séquard syndrome -
suspended dissociated sensory loss
- loss of pain and temp over the segment,
preserved sensation above and below lesion
- loss of pain and temp over the segment,
preserved sensation above and below lesion
- ASA – impaired pain and
temperature
- Course is variable
- TIA of cord lasts 15 minutes
- Slowly progressive myelopathy from chronic
constriction described
- Infarction in minutes, pain in hours (major
disabling factor)
- Return of function <24 hours is good prognosis
for recovery
- TIA of cord lasts 15 minutes
Investigations
- MRI is imaging process of choice, but can be normal
despite symptoms
- Typically shows cord enlargement, T2 hyperintensity
(8h – several days), long term atrophy
- Signal enhancement can be double dots (“owl’s eyes”)
in the anterior horns, H-shape of central grey matter, or diffuse pattern
involving grey and white
- Involvement of vertebral body if segmental artery
involved
- CSF protein can be elevated, pleocytosis is
rare
Causes
- Typical causes:
- Regional hemodynamic compromise – from disruption of
aorta, most common from AAA repair
- Systemic hypotension – especially lower cord, often
associated with encephalopathy
- Occlusive vascular disease – e.g., atherosclerotic
plaques, hyalinization – intermittent claudication
- Thromboembolism – e.g., rheumatic heart dx (mitral
valve), bacterial endocarditis, atrial myxoma
- Endovascular procedures – e.g., therapeutic renal or
bronchial artery embolization
- Fibrocartilaginous (intervertebral disc) embolism –
from ruptured disc, F>M,
- Vasculitis – radiotherapy can affect arterioles,
meningovascular syphilis
- Arterial dissection
- Thrombosis – Crohn’s, PAN, giant cell arteritis,
sickle cell, intrathecal chemicals, angiographic contrast, postpartum state,
intravascular neoplastic invasion, polycythemia rubra vera
- Venous occlusion
- Regional hemodynamic compromise – from disruption of
aorta, most common from AAA repair
- Abdominal aorta
- Clamping aorta above renal arteries >20-30
minutes, or ligation of lower vessels puts cord at risk
- AAA repair has 5-20% risk of neurological
deficits
- Aneurysmal aortic dissection also causes spinal
ischemia – grey matter ischemia, white matter adequately supplied by
longitudinal anastomotic network
- Clamping aorta above renal arteries >20-30
minutes, or ligation of lower vessels puts cord at risk
- Vertebral artery dissection – can cause posterior
cervical cord infarction
- Nonpenetrating aortic trauma – torsional occlusion of
vessels à ischemia
- Percutaneous radiofrequency spinal rhizotomy
à impaired autoregulation à local thoracic cord
ischemia
- Decompression sickness – circulating nitrogen bubbles
block small spinal arteries
- Foix-Alajouanine syndrome – subacute necrotizing
myelitis
- Stepwise spinal cord dysfunction with extensive
thrombophlebitis of spinal cord
- Associated with COPD or lung neoplasm, or end stage
chronic venous HTN and congestion (dural venous
fistula)
- Stepwise spinal cord dysfunction with extensive
thrombophlebitis of spinal cord
Treatment
- Supportive and reduce risk of
recurrence
- Maintain BP, early bedrest, reverse causes (hypoTN,
arrhythmia)
- Unclear use of acute thrombolytics or
antithrombotics
- Minimize complications of autonomic dysfunction and
immobility, PT/OT
- 20% mortality, more than minimal improvement in
35-40%
Spinal vascular
malformation
- Normal/large arteries and enlarged tortuous veins
without intervening capillary network
- Anson and Spetzler (1993) classification
system:
- Type I – dural AV fistula
- 1A – single feeding
artery
- 1B – multiple feeding
arteries
- 1A – single feeding
artery
- Type II – intramedullary glomus-type
AVM
- Type III – intramedullary juvenile-type AVM, more
extensive than a glomus-type AVM, with extramedullary and extradural
components
- Type IV – intradural, extramedullary (perimedullary)
AV fistula
- IVA, IVB, IVC – demotes progressively
increased AV shunting from increasing number, size, and tortuosity of
feeding arteries
- IVA, IVB, IVC – demotes progressively
increased AV shunting from increasing number, size, and tortuosity of
feeding arteries
- Other forms not in classification – cavernous
angiomas, venous angiomas (developmental venous anomalies),
epidural/paraspinal AVMs
Distribution and
prevalence
- Prior to selective spinal digital subtraction
angiography – often misdiagnosed as spinal tumours
- Frequency of reported spinal AVMs is 3-11%, likely
more due to asymptomatic/misdiagnosed
- Usually lower thoracic and lumbar spinal, usually
dural AV fistulas draining to surface of cord
Clinical
presentation
- Often misdiagnosed for years
- Onset can be acute or insidious, with remissions and
relapses
- Common initial complaints – pain, weakness, sensory
symptoms
- Later complaints – bowel and bladder
complaints
- Symptoms often associated with trauma, exercise,
pregnancy, or menstruation
- Locomotor difficulties in 20% after 6 months of
symptoms, 50% in 3 years
- Symptoms due to mass effect and ischemia. Epidural,
subdural, intramedullary hemorrhage cause spinal cord
compression
- Dural AV fistula rarely hemorrhages, but causes slowly
progressive myelopathy à infarction
- Pain – local, radicular, diffuse, or
combination
- Weakness – upper and/or lower motor
neuron
- Spinal bruit is specific but
uncommon
- Vascular malformations in skin sometimes
associated
- Cobb’s syndrome – cutaeomeninospinal angiomatosis – dural and
cutaneous angiomas in same dermatome
- Foix-Alajouanine – has been associated with end-stage dural AVF +
thrombosis + venous infarct
- Spinal hemorrhage – typical symptoms of spinal
SAH
- Headache, meningeal infection, cord/nerve root
damage
- CSF pleocytosis and high protein
- Headache, meningeal infection, cord/nerve root
damage
- AVM or dural AV fistulas à increased local venous pressure
à decreased perfusion pressure à ischemia
- This explains symptomatic relief from ligation of
feeding vessels
- This explains symptomatic relief from ligation of
feeding vessels
- DDx – neoplasm, herniated disc, MS, intracranial SAH,
subacute combined degeneration, meningovascular syphilis, transverse
myelitis
Investigations
- MRI with contrast enhanced MRA is test of
choice
- Intramedullary AVM
- Intramedullary low signal with surrounding normal
cord, focal cord enlargement, serpentine signal voids in subarachnoid
space.
- MRA helps detect the feeding
arteries
- Intramedullary low signal with surrounding normal
cord, focal cord enlargement, serpentine signal voids in subarachnoid
space.
- Dural AV fistula
- Slight enlargement of cord, cord hypointensity on
T1, central hyperintensity on T2, scalloping of cord, enhancement of cord on
T1
- Findings non-specific and same as neoplasm,
infection, or ischemia
- Detecting blood flow-related abnormalities important
– flow voids in T2, intradural serpentine enhancement on T1 extending >3
vertebral levels, MRA
- Selective catheter angiography is definitive gold
standard, but invasive and highly tedious
- Slight enlargement of cord, cord hypointensity on
T1, central hyperintensity on T2, scalloping of cord, enhancement of cord on
T1
Treatment
- Surgical resection and/or angiographically directed
embolisation of malformation
Spinal
hemorrhage
- Usually sudden and painful, related to trauma or
vascular malformations
Subarachnoid
hemorrhage
- Spinal SAH is <1% of all SAH
- Most common cause is spinal angioma (10%
total)
- Others: coarctation of aorta, rupture of spinal
artery, mycotic or other aneurysms of spinal artery, PAN, spinal tumours, LP,
blood dyscrasias, therapeutic thrombolytics and
anticoagulants
- Presentation:
- Sudden onset severe back pain localized near level
of hemorrhage
- In minutes, diffuse pain and meningeal
irritation
- Multiple radiculopathies and
myelopathy
- Headache, cranial neuropathies, decreased LOC – from
diffusion of blood above foramen magnum
- CSF grossly bloody, high ICP,
papilledema
- Sudden onset severe back pain localized near level
of hemorrhage
- Diagnosis:
- Clinical suspicion important
- Exam: spinal bruit, cutaneous angioma, sensory
level, collagen vascular disease, septicaemia
- Clinical suspicion important
Hematomyelia
- Intramedullary spinal hemorrhage, usually direct
spinal cord trauma or hyperextension of cervical cord
- Spontaneous hematomyelia – bleed of spinal vascular
malformation, tumour, or syrinx, bleeding diathesis, anticoagulant drugs,
venous infarction
- Disrupts grey matter > white
matter
- Not associated with hypertension or amyloid
angiopathy
- Presentation:
- Spinal shock, sudden severe back pain, radicular
pain
- Eventually spasticity below level of lesion,
fasciculations, atrophy, areflexia
- Spinal shock, sudden severe back pain, radicular
pain
- Laminectomy with drainage of hematoma, resection or
tumour/vascular malformation if deficits incomplete or
progressive
Spinal epidural
(SEH) or subdural (SSH) hemorrhage
- SEH > SSH, but clinically
indistinguishable
- SEH – more in men, and in childhood (cervical) or
50-60s (thoracic-lumbar)
- Can be spontaneous or from mild trauma, after LP or
epidural anesthesia, esp if anticoagulated
- Blood dyscrasias, thrombocytopenia, neoplasms,
vascular malformations also
- Can be spontaneous or from mild trauma, after LP or
epidural anesthesia, esp if anticoagulated
- SSH – more in women, especially 60s
(thoracic-lumbar)
- Hemorrhagic diatheses (anticoagulation, blood
dyscrasias, thrombocytopenia), trauma, LP, vascular malformation, spinal
surgery
- Hemorrhagic diatheses (anticoagulation, blood
dyscrasias, thrombocytopenia), trauma, LP, vascular malformation, spinal
surgery
- Presentation:
- Severe back pain at level of bleed
- Myelopathy or cauda equine syndrome with
motor/sensory levels develop hours-days
- Rapidly decreasing platelet count or <20,000
platelets/uL are at risk for LP (need transfusion first)
- CSF – normal, xanthchromic, or increased
protein
- MRI – delineates hematoma in the
dura
- MRI+Gad/MRA – underlying vascular
malformation
- CT myelography is alternative if patient unstable –
filling defect or blockage of contrast flow
- Does not distinguish SEH from
SSH
- Does not distinguish SEH from
SSH
- Laminectomy to evacuate clot ASAP, for better
prognosis of recovery to minimize preop deficits
- Severe back pain at level of bleed