Stroke
Ischemic stroke (85%)
- Large artery thromboembolic
infarctions
- Lacunar infarctions
- Longstanding HTN, diabetes, smoking
are risk factors
- Locations:
putamen/caudate/PLIC/thalamus, basis pontis
- Prevention by BP control, prevention
of microangiopathy, antiplatelet agents
- Cardioembolic infarctions
- Often large, multiple, wedge-shaped
- Sudden, unheralded, focal deficits
worse at onset
- Atrial fibrillation and other
arrhythmias
- Valvular disease, subacute bacterial
endocarditis, mechanical valves
- Cardiomyopathy, myocardial infarction
(esp first 1-3mo), congenital heart disease
- Cardiac shunts, patent foramen ovale,
atrial septal defect/aneurysm
- Post CABG and other cardiac surgery
(esp by POD#2)
- Intracardiac tumours
- Cryptogenic stroke
- Nonatherosclerotic vasculopathies
- Cervicocephalic dissection, traumatic
cerebrovascular disease
- Radiation vasculopathy
- Moyamoya disease
- Chronic, progressive,
nonatherosclerotic, noninflammatory, nonamyloid occlusive intracranial
vasculopathy of unknown cause
- Fibrocellular intimal thickening,
smooth muscle proliferation and elastin accumulation
- Suzuki’s 6 angiographic stages: (1)
stenosis of ICA bifurcation (2) moyamoya vessels at base of brain,
dilated ACA/MCA/PCA (3) intensification of moyamoya vessels, small
ACA/MCA (4) minimization of moyamoya vessels, small PCA (5) reduction of
moyamoya vessels, absent ACA/MCA/PCA (6) disappearance of moyamoya
vessels with extensive pial collaterals from external carotid branches
- Imaging: lenticulostriate
collaterals, Ivy sign, “puff of smoke”, narrowed
- Medical tx: ASA,
acetazolamide (vasodilation)
- Revascularization procedures:
- Direct – superficial temporal
artery to MCA bypass
- Indirect
- Encephalomyosynangiosis – muscle
flap onto brain
- Encephaloduroarteriosynangiosis –
scalp artery to brain
- Fibromuscular dysplasia
- Segmental, nonatheromatous,
dysplastic, noninflammatory angiopathy
- Young-mid aged women
- Subtypes: (1)
intimal fibroplasia (2) medial hyperplasia (3) medial fibroplasias (4)
perimedial dysplasia
- Diagnosis by cerebral
angiography – “string of beads” in extracranial carotid artery
- Vasculitis
- Migrainous infarction
- Symptoms not resolved 7 days after
imaging confirmation of infarction
- Inherited and misc disorders
- CADASIL
- Cerebral Autosomal Dominant
Arteriopathy with Subcortical Infarcts and Leukoencephalopathy
- NOTCH3 mutation – chr 19 – granular
osmiophilic material in vascular smooth muscle cells and pericytes
(GOMs) see in EM
- Ischemic episodes (lacunar),
cognitive deficits, migraines, seizures, mood disorders
- Anti-NOTCH3 Ab for diagnosis
- MELAS
- Homocystinuria or MTHFR mutation –
more like AIS
- Fabry disease
- Marfan syndrome
- Ehlers-Danlos syndrome
- Pseudoxanthoma elasticum
- Sneddon syndrome
- Livedo reticularis and
cerebrovascular accidents
- Osler-Weber-Rendu syndrome
- Lymphomatous angiomatosis
- Multiple small/medium vessel
occlusion by lymphoid neoplastic cells
- Susac disease
- Microangiopathy of brain, retina,
inner ear – retinocochleocerebral
vasculopathy
- Encephalopathy, visual loss,
vestibular dysfcn, tinnitus, vertigo, asymmetric hearing loss
- Treatment with corticosteroids,
immunosuppression, plasmapheresis, anticoagulation
- Eales disease
- Hypereosinophilic syndrome
- Cerebral amyloid angiopathy
- Arterial dolichoectasia
- Emboli - air, fat, amniotic fluid,
bone marrow, foreign body particle
- Drug abuse – ephedrine, cocaine,
amphetamine
- Hypercoagulable states
- Primary hypercoagulable states
- Antithrombin III deficiency
- Inhibits thrombin, IXa, Xa, XIa,
XIIa
- Protein C deficiency
- Vitamin K-dependent anticoagulant
- Protein S deficiency
- Cofactor of protein C
- Activated protein C resistance,
factor V Leiden mutation
- Send for mutation if APC resistance
- Prothrombin 20210 (factor II)
mutation
- Fibrinogen disorders
- Plasminogen disorders
- Antiphospholipid antibody syndrome
- Lupus anticoagulant and
anticardiolipin antibodies
- Arterial ischemic strokes, also
CSVT, migraine, vascular dementia, chorea, transverse myelopathy, fetal
loss, livedo reticularis
- Warfarin with INR>3, during
pregnancy use prednisone and low ASA
|
AIS |
CSVT |
|
Hyperhomocysteinuria Antiphospholipid
antibody syndrome Protein
C deficiency (chr2) Protein
S deficiency (chr3) Lipoprotein
(a) |
Prothrombin
20210 mutation (chr11, AD) Antithrombin
III deficiency (chr1) Factor
V Protein
C deficiency (chr2, AD) Protein
S deficiency (chr3, AD) Antiphosholipid antibody
syndrome Hyperhomocysteinuria |
·
Secondary
hypercoagulable disorders
- Malignancy
- Pregnancy, puerperium, OCP use
- Sickle cell disease
- Polycythemia
- Thrombocytopenia
- HIT (heparin induced
thrombocytopenia)
- Type I – mild, benign condition
with platelet counts 100,000/mcl
- Type II – delayed onset (5-15d),
severe, requires d/c heparin
- Prevent by limiting exposure to
<5d heparin
- Daily platelet counts
- TTP (thrombotic thrombocytopenic
purpura)
Stroke risk factors
|
Non-modifiable factors |
Modifiable factors |
|
Age - strongest risk factor, 50%
strokes >70 years age Gender Race/ethnicity Family history Genetics |
Arterial hypertension - 3-4x increased risk, drop
SBP by 10 or DBP by 5 Transient ischemic attacks Asymptomatic carotic
bruit/stenosis Cardiac disease Aortic arch atheromatosis Diabetes mellitus - 2-4x increased risk,
additive with age or BP Dyslipidemia - high cholesterol, high LDL,
low HDL Cigarette smoking - 2-3x increased risk,
baseline by 5 years of quitting Alcohol consumption - 2 drinks/day good, >2
drinks/day bad High fibrinogen High homocysteine Low folate High anticardiolipin
antibodies Oral contraceptives Obesity (esp. truncal
obesity) |
HOPE trial – controlling HTN in DM results in 1/3 RRR in
stroke
4S (Scandinavian Simvastatin Survival Study) in cardiac patients –
post-hoc ½ RRR in stroke, 1/3 RRR in TIA
CARE trial – statins in CAD patients 1/3 RRR in stroke
SPAF (Stroke Prevention in Atrial Fibrillation)
- <65, no
risk factors – ASA
- 65-75, no
risk factors – ASA or warfarin
- >75 and
anyone with risk factors – warfarin
- Afib + ASA =
20% RRR
- Afib +
warfarin = 65% RRR
ACST (Asymptomatic Carotid Surgery Trial)
ACAS (Asymptomatic Carotid Atherosclerosis Study)
- <75%
stenosis – 1.3% risk of stroke
- >75%
stenosis – 10.5% risk fo stroke
- Trials looked
at >60% stenosis, medical vs. surgical management
- Need very
low risk perioperative mortality to go to surgery
NASCET (North American Symptomatic Carotid Endarterectomy Trial)
- Risk of
stroke after TIA – 8.5% at one week, 20% at 90 days (1/2 for retinal TIA)
- With carotid
stenosis (70-99%) and TIA – 25% at 90 days
Antithrombotic Trialist Group (metaanalysis)
- Long-term
risk reduction in cardiovascular events 22% risk reduction with
antiplatelets
- 2.5% ARR,
23% RRR in stroke after TIA/stroke with ASA
Weird syndromes:
- Subclavian steal – reversal
of flow of vertebral artery due to subclavian stenosis or occlusion of
proximal vertebral artery or brachiocephalic artery, especially from left
- Transient global
amnesia – reversible anterograde/retrograde amnesia,
lasting 3-6 hours, more in men >50 years, triggered by physical
exertion, temperature, or sexual intercourse
Dr.
Silver’s review session
- Stroke
prevention outcome is for disability and dementia, and not so much death
as in MI
- Stroke
incidence increases with age, and is more common than MI
TIAs
- 90
day risk of stroke after TIA is 10%
- ABCD2 rule
- A – age 60+ (1pt)
- B – blood pressure
SBP>140 (1pt)
- C – TIA features –
unilateral weakness (2pts), speech impairment w/o weakness (1pt)
- D – duration of TIA –
10-59min (1pt), 60+min (2pt)
- D – diabetes (1pt)
- Low (0-3, 1% risk),
moderate (4-5, 4% risk), high (6-7, 8% risk) stroke in 48hrs
- MRI
showing DWI lesion increases risk of re-stroke, if also vessel occlusion
then 30% risk of restroke
- EXPRESS
trial – 2007 (
- Historical
control compared to last few years of rapid workup and
clopidogrel+ASA+ACEinh
- Dramatic
improvement in risk of restroke
- Another
trial in
Acute Stroke
- Neuroprotection
and thrombolysis
- Early
CT signs of stroke
- Hyperacute
MCA sign, or other vessel
- Subtle
decreased grey-white differentiation
- Early
mass effect – sulcal effacement and shift
- ASPECT scoring (
- Lower cut – M1, M2, M3,
Caudate, Lentiform
nuclei, Internal Capsule, Insula
- Upper cut – M4, M5, M6
- Good prognosis if
score >7
- Perfusion/diffusion
mismatch
- Diffusion
is area that is edematous
- Perfusion
is area that has less blood supply
- >20%
mismatch is significant – the penumbra
- Neuroprotection
- Hypothermia
- Avoiding
hypotension, hyperglycemia, fever, seizures
- Retard
ischemic cascade, e.g.,
glutamate antagonists, NOS antagonists, free radical scavengers? - Check
American Heart Association guidelines for BP management
- Hemicraniectomy
(ideally 12-24 hours after event)
- 30
day mortality of large MCA stroke is 80%
- Edema
peaks at 72 hours
- Hyperventilation,
mannitol, hypertonic saline – too short acting
- Combination
of 3 trials (93 patients), “good” outcome mRS 0-4
- Limited
inclusion criteria (<60yrs, NIHSS>15, 50%+ MCA involvement)
- Mean
time to treatment was about 15-30 hours
- 55%
RRR of poor outcome, for either hemisphere
- NINDS
trial (1995)
- Inclusion
criteria
- <3 hours
- clearly defined, stable deficit
- CT no hemorrhage
- No seizure at onset
- BP<185-110
- No recent surgery, hemorrhage, stroke
- Informed consent (no longer necessary, now is standard of care)
- Outcome
- 11% absolute benefit
- 55% relative benefit
- 0.6 becomes 6.4% hemorrhage rate
- NNT 10 for good outcome
- tPA approved in Canada in 1999
- PROACT
II trial (1999)
- Prourokinase,
no longer available, tested in angiography-proven occlusions
- NNT
7 for good mRS outcome, 15% patients reached independence
- 6
hour treatment window, average 5.5 hour treatment, 2 hour treatment
course
- Pooled
analysis of tPA 0-6 hours (2004)
- 3000
patients, mean NIHSS 11, 1/3 treated
- Favorable
outcome of mRS 0-1
- The
longer you wait before treatment, the less probability of good outcome
- 300
minutes when no risk improvement compared to controls
- Delayed
treatment NOT associated with risk of bleeding
- Risk
of death only after 270 minutes
- IMS
trials (Interventional management of stroke study)
- IV
rtPA 0.6mg/kg, 15% bolus, followed by angiography, up to 22mg IA rtPA
over 2 hours
- CASES trial (Canadian Activase for
Stroke Effectiveness Study, 2005)
- 4.6% symptomatic
intracerebral hemorrhage
- 1.3%
anaphylactoid/angioedema reactions – swelling is ipsilateral to
hemiplegia, more risk if patient of ACEinh
- Atrial fibrillation as
cause of stroke was found to be a good outcome predictor
- SIT-MOST
(Safety Implementation of Thrombolysis in Stroke)
- Devices
for mechanical thrombolysis
- Merci
– physically impressive, but unclear if good evidence of clinical
efficacy
- Ekos
– transcranial Doppler during tPA helps activity of tPA (physical
agitation)
- FASTER
- Clopidorel+ASA vs. ASA
(also looked at simvastatin)
- Trend towards
combination therapy preventing more strokes
- PRoFESS
- Aggrenox
vs. Plavix
- Micardis
vs. placebo
- CREST
- Carotid
endarterectomy vs. stenting
Secondary stroke prevention
- NASCET
trials
- Carotid
endarterectomy in symptomatic disease
- Consider
if >50% stenosis, definitely treat if 70-99%
- Ideally
treat within 2 weeks
- Stenting
with distal protection device
- SAPPHIRE
trial – stenting better than endarterectomy if including MI, stroke,
mortality
- Restenosis rate in stenting 20%, CEA 31%
- EVA-3S
trial – stenting
- Outcome worse, but also ? experience of interventionalists
- SPACE
trial
- No difference between stenting and endarterectomy
- CREST
trial (NIH-Canada)
- Ongoing trial of carotid endarterectomy and stenting
- Both symptomatic and asymptomatic patients included
- Warfarin
in A fib
- 80% RRR of use of warfarin in patients with a. fib
- In patients >80 years, 25% strokes due to a fib
- CHADS score
- CHF (1pt)
- Hypertension (1pt)
- Age >75 (1pt)
- Diabetes (1pt)
- Stroke/TIA (2pts)
- 0 (low), 2 (moderate), 4+ (high) risk
- Antiplatelet
agents
- ASA
- Dipyridamole
- Ticlopidine
- Clopidogrel
- GpIIb/IIIa antagonists
- Combination therapies
- Aggrenox (diapyridamole+ASA)
- Clopidogrel+ASA
- Irreversible inhibition of platelet activation and aggregation
(except dipyridamole)
- Antithrombotic Trialists’ Collaboration (2000)
- Antiplatelet agents result in strong protection against
re-stroke
- Dose of ASA not important (minimum 30mg/day)
- CAPRIE trial
- Clopidogrel 75mg vs.
ASA 325mg
- Stroke, MI,
peripheral
- Small improvement in
reduction rate of events – 9% RRR
- Decreased risk of
bleeding
- MATCH trial
- Clopidogrel/ASA vs. Clopidogrel
- No significant difference, trend to helpfulness in acute (7d)
setting
- Increase in bleeding longterm treatment
- CHARISMA trial
- Clopidogrel/ASA vs. ASA
- No significant benefit
- Aggrenox
- Containts a tartaric acid core, dipyridamole requires acid
environment to be absorbed, thus issue in patients on H+ blockers
- ESPS trial (European)
- ASA vs. dipyridamole vs. combo vs. placebo
- Clear improvement in stroke-free survival with treatment, esp
combo
- ESPRIT trial (European/Australasian, 2006)
- ASA vs. dipyridamole/ASA
- 20% RR with combination treatment, decreased bleeding
- Warfarin
- WARSS trial
- Warfarin vs. ASA in
noncardioembolic stroke
- No benefit, more
complications
- WASID trial
- Warfarin vs. ASA
for symptomatic intracranial arterial stenosis
- Stopped due to
increased harm
- Anticoagulation
- Cardioembolic stroke
- Acute arterial dissection
- Progressive stroke with documented large artery occlusive
disease, e.g., basilar
- Sinovenous thrombosis
- Risk factor modification
- ACE inhibitor or ARB (+BP
control)
- PROGRESS trial – perindopril + indapamide
- Quit smoking
- Manage diabetes
- Statins
- SPARCL study – significant reduction in LDL
- 16%RR of stroke despite unintended treatment of placebo
patients with statins
- 35% RR coronary events despite CAD patients being excluded
from trial
- Folic acid
Cerebral sinovenous thrombosis
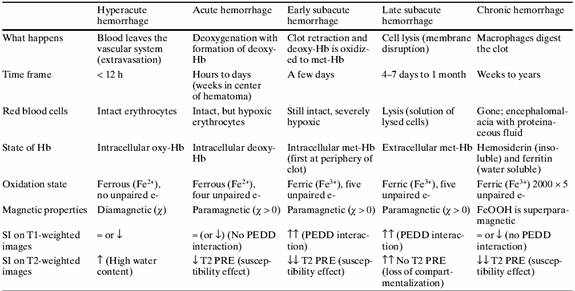
Hemorrhagic infarct
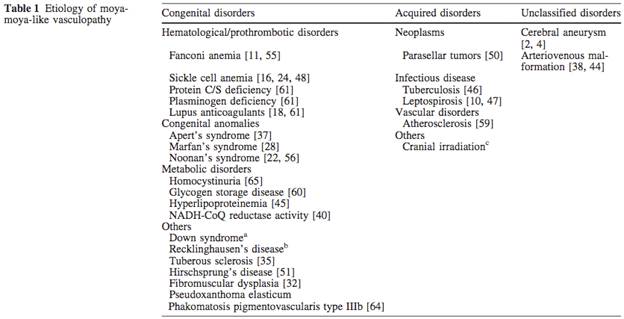
- Etiologies:
- Amyloid angiopathy - lobar
- Hypertensive angiopathy – thalamus,
basal ganglia, brainstem, cerebellum
- Cocaine
- Malignant hypertension
- Reversal of coagulopathy
- Protamine sulphate to reverse heparin
- Vitamin K to reverse warfarin
- FFP to normalize INR
- Surgical decompression in 12-24 hours
for:
- Cerebellar/brainstem hemorrhage
>3cm
- Clots causing hydrocephalus
- Superficial location
|
CT appearance |
» heterogeneous |
|
|
(enhancing edge, fluid-fluid level) |
¯ (hemosiderin-lined, calcification) |
Vascular malformations
- Vascular malformations without AV
shunts
- Developmental venous anomalies (DVA)
- Venous structure, no arterial
involvement
- Arrest of fetal venous development
- Usually incidental finding, can be
seen in seizures/headache
- “Caput medusa” appearance on imaging
from radial draining veins
- Capillary telangiectasia
- Small groups of abnormally dilated
capillaries, often in pons
- Rarely hemorrhage, found only
postmortem
- Venous cavernoma
- Majority are clinically silent and
undetectable by angiography
- Can present with seizures or focal neurological
deficits, 2-3%/yr risk hemorrhage
- “Popcorn” appearance on MRI
- Vascular malformations with AV shunts
- Cerebral (subpial) AV malformation
- Commonly present 20-30 years
- High flow AV shunting resulting in
arterial hypotension
- Wedge-shaped tangle of arteries and
veins without intervening capillaries
- Common presentation: hemorrhage,
seizures, headache
- Can show focal deficits, progressive
cognitive decline, cardiomegaly, hydrocephalus
- Natural history:
- Annual risk of hemorrhage – 2-4%
- Mortality from 1st bleed
– 5-15%
- Risk of bleed recurrence – 6% in
first year, 2-4% annually
- Mortality from 2nd bleed
– 5%
- Surgical options:
- Stereotactic radiosurgery – for
small, deep, highly vascular AVMs, 2yr to effect
- Endovascular embolization – for
larger AVMs, immediate effect
- Dural AV fistula
- Vein of Galen malformation
- High pressure vascular communication
between major cerebral arteries and vein of Galen
- Fistulous connection between
primitive choroidal vessels and embryonic median prosencephalic vein of Markowski
- Causes high-output congestive heart
failure, failure to thrive, hydrocephalus
- Treatment: endovascular embolization
Intracranial aneurysms
- 80-85% anterior circulation
- Internal carotid, anterior
communicating, posterior communicating arteries
- Trifurcation of MCA
- Posterior circulation
- Bifurcation of basilar artery
- Vertebral artery/PICA junction
- 0.5-2% annual risk of rupture, 2% risk
of new aneurysm after rupture
- Risk factors:
- Connective tissue disorders:
- AD polycystic kidney disease
- Ehlers-Danlos type IV
- NF type 1
- Marfan syndrome
- Familial aneurysms – higher risk of
rupture and new aneurysms
- Smoking – via alpha-1-antitrypsin
inhibition
- Hypertension
- Moderate-high alcohol consumption
- Post-menopausal without HRT
- Presentation:
- Subarachnoid or intracranial
hemorrhage
- Sudden severe headache, loss of
vision, nausea/vomiting, loss of consciousness, CN3 palsy
- Management:
- Early surgical clipping decreases
risk of recurrence and ischemia from vasospasm
- Endovascular coiling